This winter season avalanches unfortunately already caused some victims. The number of fatalities in the Alps due to avalanches this season already is well over twenty. In mountainous areas during the winter, the risk of avalanches is real for anyone and it can strike anywhere: it can happen to a group of backcountry skiers in a remote area or a young daredevil who just runs off-piste for a little patch of tiefschnee. Previously, five tips were given on how to recognize avalanche terrain and what equipment is necessary before skiing off-piste sections. Should someone nevertheless end up in an avalanche, quick help is essential. This article briefly outlines what to do if someone becomes an avalanche victim. This is not intended to replace any kind of course; rather, it is intended to show how much skills and practice is involved. So taking a proper course is highly recommended before you choose to set those first tracks.
Pathophysiology
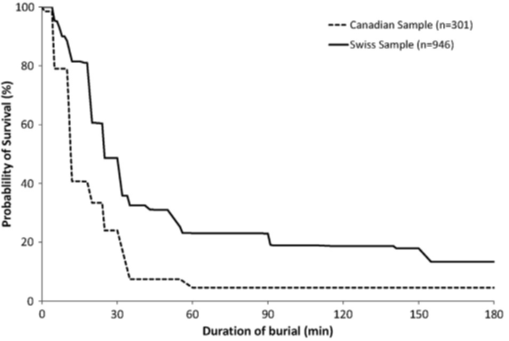
In Europe, approximately 100 avalanche-related deaths happen each year.1 As mentioned, quick help is needed and there is no time to waste for the emergency services to arrive. The chances of someone making it out alive after being buried for more than 10 minutes, decreases significantly by the minute due to asphyxia. This is the cause of death in about three quarter of the victims. If someone can be dug up within these critical 10 minutes, the chance of survival is about 90%. After 30 minutes, this chance is only 30% (see Fig. 1). Victims who survived longer had a free airway and a (large) airpocket.2 As any medic knows, prevention is better than cure. Using an avalanche airbag decreases the chance of becoming fully buried. An avalung regulates disposal of CO2, postponing rebreathing hypercapnic air. Both devices can be used to prevent asphyxia.
Aside from asphyxia, the last quarter dies from the traumatic injuries sustained. Common injuries include brain injuries, spinal damage, and fractures of the long pipe bones.2
Only a small proportion dies from the effects of hypothermia, provided that a patient can breathe sufficiently, for example by having a big air pocket or having its head raised above the snow. Although hypothermia has proven to be neuroprotective, the environment an avalanche victim is put into has some extra detrimental factors. With an air pocket one has a dead air space ventilation. This causes hypoxia but more importantly also hypercarbia. Hypothermia in combination with hypoxia and hypercarbia (triple H- syndrome) may result in a worse neurological outcome.3 Nevertheless, hypothermia starts to play a major role after a person is dug out. After all, being buried, the snow provides a thick, admittedly cold, layer of insulation. The victim will be wet from the melted snow due to their own body temperature and when exposed to the cold air, the person will cool down rapidly. In the process, the afterdrop will contribute to a fast falling core temperature (cooled blood from extremities will end up centrally through movement and activation).4,5
How does a rescue operation take place
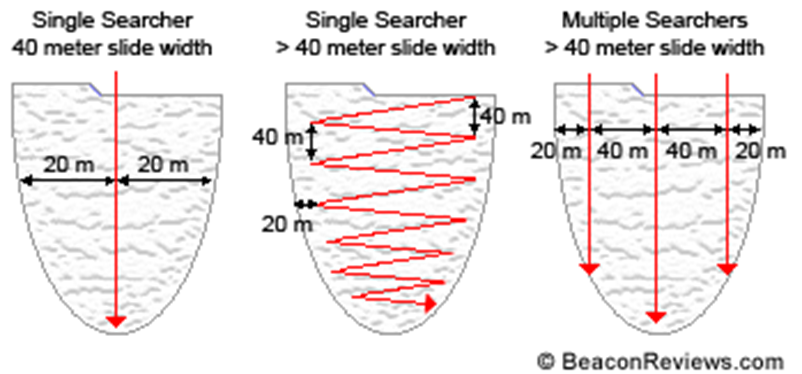
An avalanche victim is completely dependent on help from others, mostly being its uninjured companions since they are nearby. From this group, one person is designated as the leader. With an eye out for their safety, a rescue plan is drawn up. Ideally, there is one person who continues to screen the surrounding area for potential danger (after all, there could always be a second avalanche). If the rescuers are uphill from the victim they will begin searching from the point where they saw the victim last going downwards. If the rescuers are downhill from the avalanche, they will start searching from the end of the debris going upwards. The search consists of picking up signal, locating signal, probing, and shovelling. Mountain rescue should also be called in quickly, but don’t let this get in the way of the initial search! Before picking up the signal everyone sets its avalanche beacon to “search”, in that way only the victim is “sending” a signal. Avalanche beacons have a certain range, which can range from 10-50 meters and sometimes more. This is indicated on the beacon. As long as no signal is received, the avalanche debris will have to be screened without missing sections or double-screening sections. Which pattern to use depends on the size of the debris field and the number of searchers. If you are alone you will search in a zig-zag pattern, if you are with a larger group you may walk side by side in a straight line (see fig. 2).
Once a signal is received, the beacon indicates the direction and distance to the victim. At the strongest signal, the probe can be used to locate the victim. To avoid too many unnecessary probes (which wastes time), this is also done in a certain pattern (see Fig. 3). The probe can also be used to determine the depth to the victim. Shovelling should be started downhill from the probe. For a victim lying shallow (< 1 meter), shovelling can be done as quickly as possible toward the victim. When a victim lies deeper one has to consider that a big volume of snow will need to be shovelled. In this case, one or two shovelers will focus on the victim’s location, the other(s), will shovel the shovelled snow further downhill. This simultaneously creates a path of 1-2 meters wide through which the victim can be evacuated (see Fig. 3). Note that shovelling is heavy. Make sure there is enough rotation to keep up the speed.

When the victim is reached, excavate the head as soon as possible and ensure a free airway. When necessary the first ventilations can already be given and CPR can be started when the head and thorax are excavated.
Care of the victim should follow the familiar ABCDE or MARCH method, with extra attention to a free airway, traumatic injury, and hypothermia. A fully buried casualty should be taken to the hospital for checks. Even though a victim may look fine, hypothermia and/or an afterdrop may still cause problems. In rare cases, a patient develops hypoxemia-induced heart failure or pulmonary edema, possibly due to the pulmonary negative pressure that originates with a blocked airway. Traumatic injuries resulting from the avalanche should be treated by regular medical means.
With the increasing interest in freeriding and backcountry skiing, more people are at risk of getting caught in an avalanche. Once someone is caught, time is limited and a quick rescue is essential. Executing a proper rescue, requires proper training. Make sure you take an avalanche course before you set foot in the tantalizing powder.
Do you want to combine such training with a course on providing acute medical care in the mountains in winter conditions? Then sign up for our Mountain Medicine Winter edition!
In case you want to impress your fellow course participants, have a look at this!
References
- European Avalanche Warning Services
- Van Tilburg et al., ‘Wilderness Medical Society Practice Guidelines for Prevention and Management of Avalanche and Nonavalanche Snow Burial Accidents’, Wilderness Medical Society Practice Guidelines, 2017
- 3. Woyke S et al., ‘Effects of Carbon Dioxide and Temperature on the Oxygen-Hemoglobin Dissociation Curve of Human Blood: Implications for Avalanche Victims’, Frontiers in Medicine, 2022
- AWLS, Advanced Wilderness Life Support, Textbook Edition 9.0 Copyright 2016 by AdventureMed, LLC
- Podcast: Advanced Wilderness Life Support: Avalanche, University of Utah, 2020
- Backcountry Beta: Episode 3—Probing and Shoveling
- Notfall Lawine | SicherAmBerg Skitouren

